Thanks to Wayne Lusvardi @ LewRockwell.com.
Back on March 11, I wrote a preliminary article on the causes of the death of Bill Sardi, a fixture on Lewrockwell.com and across the nation on natural approaches to health and an ardent antivaxxer. At that time, I believed the public needed an explanation of his death, especially if it was attributed to Covid-19 as Bill asserted Coronavirus-19 was a “hoax”. I was careful to say at that time: “The above is a preliminary opinion subject to change when there is better information and the availability of medical records for review”. My best non-expert assessment then was that Bill died of pulmonary embolism coupled with coronary artery disease, pneumonia and hypoxia. I offer here an update now that an official death certificate showing the causes of death has been obtained. Moreover, Bill Sardi’s death reveals the actual cause of death from the bugaboo Covid-19 as Sepsis from hospitalization.
The official causes of Bill Sardi’s death are listed as follows:
Immediate cause: Sepsis
Sequential underlying causes: Pneumonia, Covid-19
Other significant conditions: Coronary artery disease, Pulmonary embolism
I spoke with a doctor who requested to remain anonymous about the above causes of Sardi’s death. He said listing COVID-19 as the third cause of death is highly impossible given that Bill Sardi had four consecutive negative PCR antibody tests, two before entering the hospital and two after admission. Reportedly, Sardi had a positive PCR test after about two weeks in the hospital but that could have been because of Sepsis staph infection (mostly incurable staph), not Covid-19.
Covid-19 is All About Sepsis
Sepsis is reported to be the leading cause of death in hospitals and is typically attributed to bacterial infection. Sepsis is associated with co-morbidities (diabetes, coronary artery disease, kidney failure, etc.), but sepsis can be acquired in hospitals independent of co-morbidities of the elderly, such as in children.
According to Jean-Louis Vincent, MD, PhD, Belgium, Covid-19 cannot be distinguished from sepsis. Sepsis can be acquired from staph (superbug MRSA – Methicillin Resistant Staphylococcus Aureus) infections that typically develop when a patient’s lung is ventilated for a lengthy period. Tracheotomy is one possible method of circumventing mechanical ventilation and was considered for Bill Sardi, but then never implemented. The long-term prognosis of tracheotomy is not positive, however. Moving Sardi out of the hospital to another hospital with a lower Sepsis infection rate was advocated by Front Line Doctors and Sardi’s advocates, but the opposition of the person with medical Power of Attorney for Sardi thwarted that effort.
Antibiotics supercharge staph germs. Another way to say this is the only way to get MRSA-Sepsis is to be exposed to antibiotics. Deadly staph bacteria normally reside on the top of one’s skin and is harmless unless one is stuck with an un-swabbed needle, a urinary catheter is inserted, or the lung is put on a ventilator. Or if a patient is awake and alert and served meat that has been raised on antibiotics, deadly bacteria may also develop. The longer one stays in a hospital the greater the likelihood of deadly sepsis. So, the selection of a hospital with a low MRSA infection rate is all-important.
The French medical diagnostic experts Bio-Force (bioMerieux) report that one hundred percent (100%) of Covid-19 non-survivors had Sepsis and “viral infections do not generally cause sepsis”. Contrary to the official notion that the bugaboo Covid-19 is a virus, sepsis is a bacterial disease, not typically a viral disease. So, the cleanliness of a hospital matters when hospitalized with the bogey Covid-19.
Both Sides Get It Wrong About Covid-19
The public do not get their medical knowledge or opinions by reasoning; they catch them by social contagion, typically along politicized social class lines separating the Knowledge Class and the Working Class. So, the Left believes that Covid-19 is a real virus that has caused death rates to rise and that vaccines are its only antidote. The Right believes that COVID-19 is a hoax, is not contagious and vaccination is a social marker (or secular circumcision) for those inside the government club. The Left pushes vaccines, boosters, hospitalization and Remdesivir. The Right pushes avoidance of vaccines, Remdesivir and hospitalization and prevention by hydroxychloroquine and Ivermectin. Both do not address the potential danger of the MRSA infection rate of different hospitals as all-important.
The case of Bill Sardi illuminates that COVID-19 is a hoax, as he claimed it was and that the cause of all COVID-19 deaths is Sepsis from hospitalization. There is some evidence, however, that Hydroxychloroquine and Ivermectin prevent death from Sepsis. But Hydroxchlorquine and Ivermectin are advocated as a preventative not for critical care.
The HAT Protocol has been shown to have success in treating Sepsis and entails: hydrocortisone (a steroid hormone), intravenous Vitamin C (up to 6,000 mg/day without conversion to oxalate) and Thiamine Vitamin B-1 (Thiamine). No treatment protocol, however, may be able to overcome the Sepsis superbug.
The reality that both sides ignore is that there is no effective medical treatment for Sepsis (MRSA or staph) once acquired in a hospital. But hospitals do not want to be accused of doing nothing, so they throw the proverbial “kitchen sink” of (deadly) drugs and tranquilizers, treatments (ventilation, intubation) at the patient. Once hospitalized one’s survival rate depends more on the highly variable infection rate of Sepsis from hospital to hospital than from Covid-19.
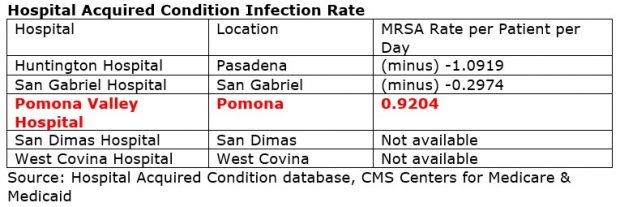
The selection of a hospital is often made by the local Fire Department ambulance dispatcher depending on which hospital has a bed in the Intensive Care Unit (ICU) at that time, not necessarily by the patient or alternate person with medical Power of Attorney (POA). Below is the infection rate for Pomona Valley Medical Center Hospital where Sardi died compared with other nearby hospitals:
Link – https://data.cms.gov/provider-data/dataset/yq43-i98g
Pre-Covid in 2019 Pomona Valley Medical Center Hospital was widely known to have a poor infection grade (see: Pomona Valley Hospital Still Struggles with Infection Rates, Daily Bulletin newspaper, May 7, 2019).
What does the MRSA Sepsis infection rate mean and how is it calculated? It means the clinical disease rate per 1,000 patient days or: total positive clinical cultures (or MRSA BSI) divided by total inpatient days, times 1,000 days. Most readers eyes will gloss over the numbers and want to know what it means. But Huntington Hospital had an effectively zero Sepsis infection rate for MRSA Sepsis. As one anonymous doctor told me: “if Sardi had been brought to Huntington Hospital in Pasadena instead he would probably still be alive today”. Pomona Valley Hospital has a total of 91,704 patient days per year tentatively indicating 84 sepsis deaths per year if I have calculated this correctly.
Pomona Hospital has a Total Performance Score (TPS) of 24.75 while the average is 37. Huntington Hospital has a TPS score of 79.4 and nearby Arcadia Methodist Hospital 72.2.
The moral of this story is that it is the hospital MRSA infection rate that is apparently more important than whether a patient was given the potential “deadly” Remdesivir or denied Hydroxychloroquine or perhaps even ventilated. All such treatments are included in the Standard of Care, so hospitals have no liability for using them within established dosages and procedures in life-or-death situations; unless the designated POA objects to their use.
This also means that those persons designated as having medical Power of Attorney, at minimum, must have enough knowledge to steer the patient to a hospital with the lowest MRSA infection rate available. The Hospital Acquired Condition database can be accessed at https://data.cms.gov/provider-data/dataset/yq43-i98g
Nothing in this article should be construed as medical advice and is entirely subjective opinion.
